JCM, Free Full-Text
Por um escritor misterioso
Last updated 18 fevereiro 2025
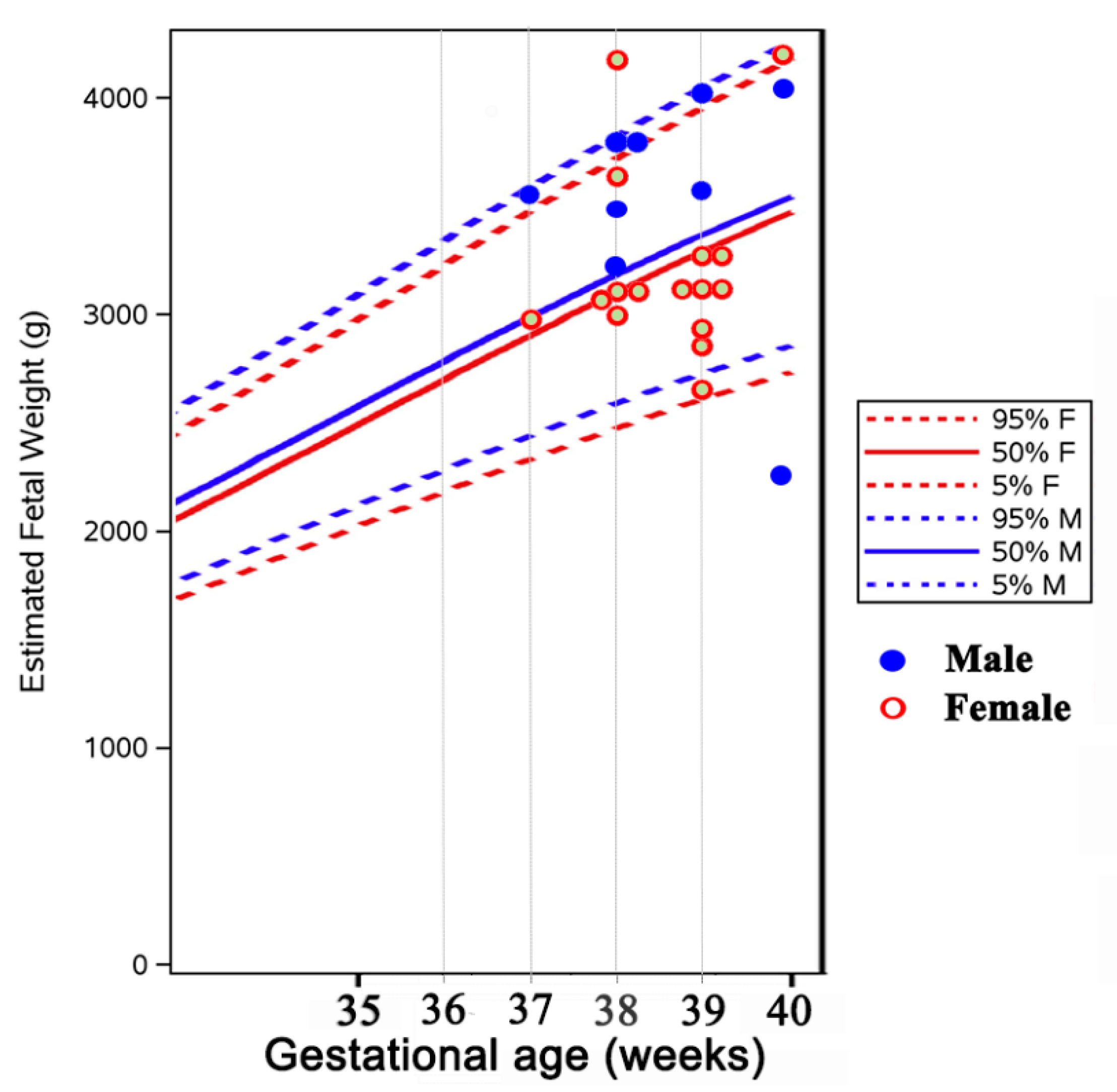
Overt hyperthyroidism (HT) during pregnancy is associated with a risk of maternal–fetal complications. Antithyroid drugs (ATD) have a potential risk for teratogenic effects and fetal–neonatal hypothyroidism. This study evaluated ATD treatment and thyroid function control during pregnancy, and pregnancy outcome in women with HT. Patients and methods: A retrospective analysis of 36 single fetus pregnancies in 29 consecutive women (median age 30.3 ± 4.7 years) with HT diagnosed before or during pregnancy; a control group of 39 healthy euthyroid pregnant women was used. Results: Twenty-six women had Graves’ disease (GD, 33 pregnancies), 1 had a hyperfunctioning autonomous nodule, and 2 had gestational transient thyrotoxicosis (GTT). Methimazole (MMI) was administered in 22 pregnancies (78.5%), Propylthiouracil (PTU) in 2 (7.1%), switch from MMI to PTU in 4 (14.2%), no treatment in 8 pregnancies (3 with subclinical HT, 5 euthyroid with previous GD remission before conception). In the 8 pregnancies of GD patients diagnosed during gestation or shortly before (<6 weeks), i.e., with fetal exposure to uncontrolled HT, there was 1 spontaneous abortion at 5 weeks (3.4% of all ATD-treated pregnancies), and 1 premature delivery at 32 weeks with neonatal death in 24 h (3.4%); 1 child had neonatal hyperthyroidism (3.3% of live children in GD women) and a small atrial sept defect (4% of live children in ATD treated women). In women treated more than 6 months until conception (20 pregnancies): (a) median ATD doses were lower than those in women diagnosed shortly before or during pregnancy; (b) ATD was withdrawn in 40% of pregnancies in trimester (T)1, all on MMI < 10 mg/day (relapse in 14.2%), and in up to 55% in T3; (c) TSH level was below normal in 37%, 35% and 22% of pregnancies in T1, T2 and T3 respectively; FT4 was increased in 5.8% (T1) and subnormal in 11.75% in T2 and T3; (d) no fetal birth defects were recorded; one fetal death due to a true umbilical cord knot was registered. Mean birth weight was similar in both ATD-treated and control groups. Hyperthyroidism relapsed postpartum in 83% of GD patients (at median 3 ± 2.6 months). Conclusion: In hyperthyroid women with long-term ATD treatment before conception, drugs could be withdrawn in T1 in 40% of them, the thyroid function control was better, and pregnancy and fetal complications were rarer, compared to women diagnosed during pregnancy. Frequent serum TSH and FT4 monitoring is needed to maintain optimal thyroid function during pregnancy.

The Best Gifts for History Buffs - Unique Gifts for History Buffs

JCM Telecom

Hire: Marshall JCM800 Head — Studiocare
Smart View 11.1 2.5 610 - Colaboratory
Home
JCM800 - SabroTone
JMH Mummy Font Download

Marshall JCM2000 Triple Super Lead 100 Head

Kajabi: Create and sell online courses, coaching, and memberships

Triple Super Lead JCM-2000 TSL 100 Ampl/Mixer Marshall, Jim
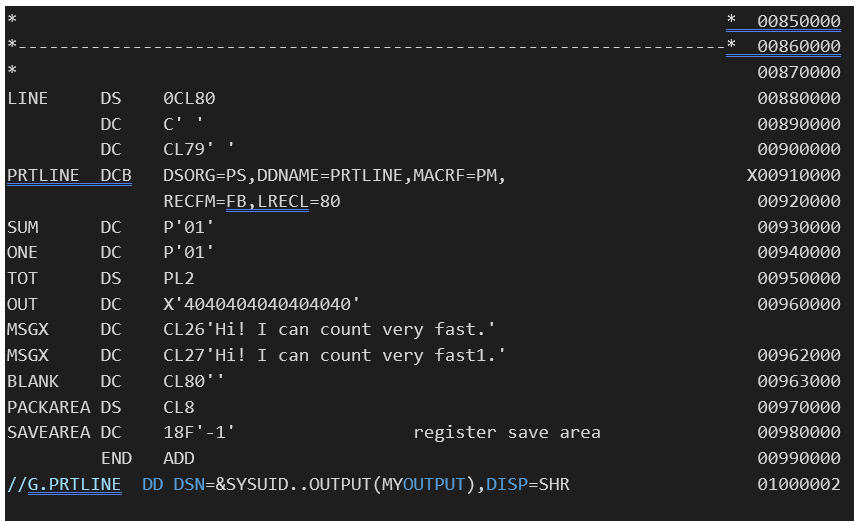
Solved Please Help Need ASAP Assembly Language Upload the

Jeff Collins Ministry
Recomendado para você
-
 A dagger M 37 for leaders, manufacturer M 7/36, E. & F. Hörster, Solingen Very good bright blade, the obverse with etched motto Blut und Ehre! (Blood and Honour!), the reverse etched18 fevereiro 2025
A dagger M 37 for leaders, manufacturer M 7/36, E. & F. Hörster, Solingen Very good bright blade, the obverse with etched motto Blut und Ehre! (Blood and Honour!), the reverse etched18 fevereiro 2025 -
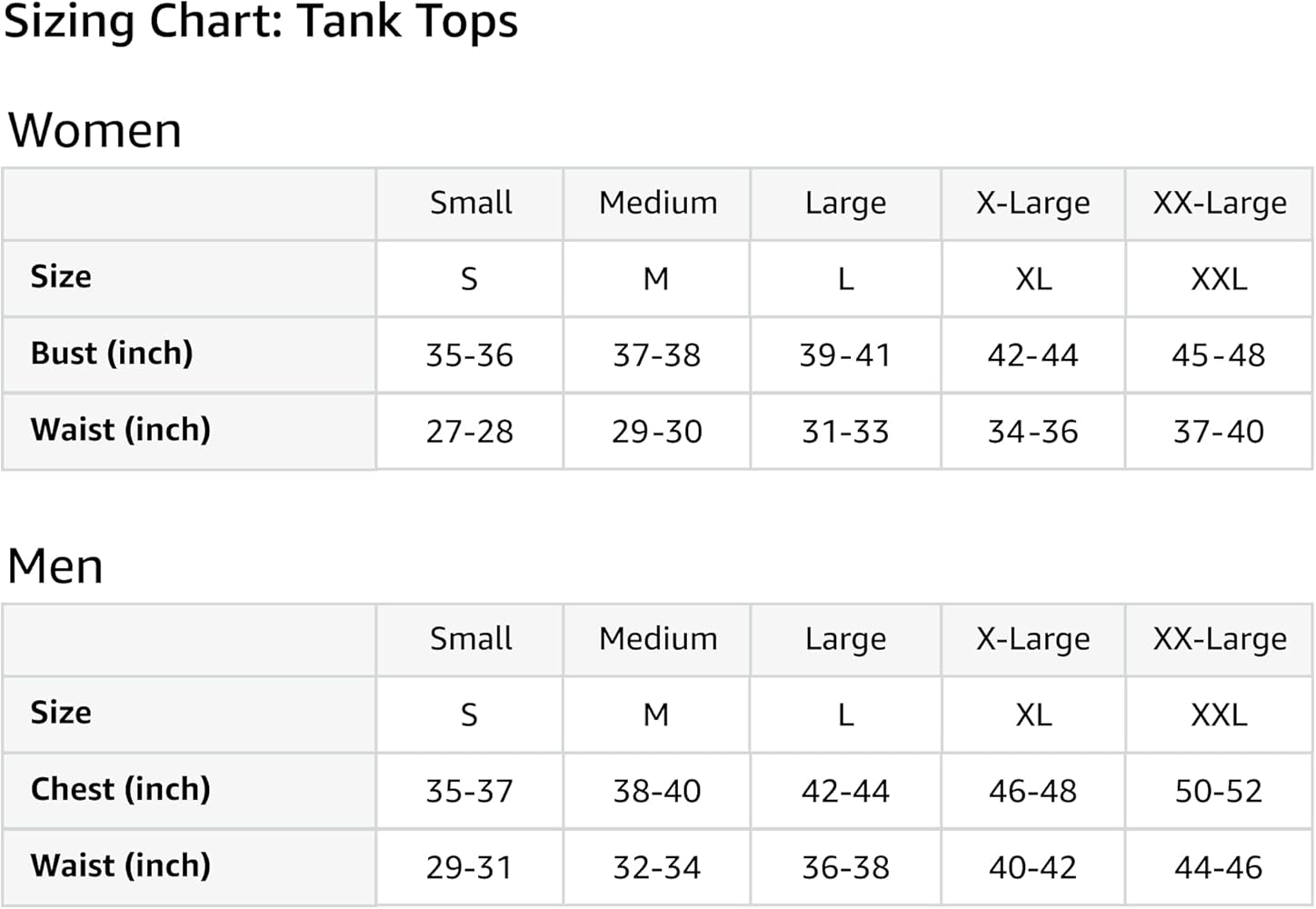 What The F, Aperture Photography Tank Top : Clothing, Shoes & Jewelry18 fevereiro 2025
What The F, Aperture Photography Tank Top : Clothing, Shoes & Jewelry18 fevereiro 2025 -
 Demonstrations of the manipulator used for 3D printing in construction.18 fevereiro 2025
Demonstrations of the manipulator used for 3D printing in construction.18 fevereiro 2025 -
 Embraer EMB-314/A-29 Super Tucano with Armor Plate by StarEagle711 on DeviantArt18 fevereiro 2025
Embraer EMB-314/A-29 Super Tucano with Armor Plate by StarEagle711 on DeviantArt18 fevereiro 2025 -
 T.E.A.M on X: Fantastic 2nd place finish for #CarrieVerdon @CUCB 10M race. She is slowly getting more confident in her ability every race! Great race also by @GeeLee_21! Has had a couple18 fevereiro 2025
T.E.A.M on X: Fantastic 2nd place finish for #CarrieVerdon @CUCB 10M race. She is slowly getting more confident in her ability every race! Great race also by @GeeLee_21! Has had a couple18 fevereiro 2025 -
 Table 1 from Alternative Treatment of Osteoma Using an Endoscopic Holmium-YAG Laser18 fevereiro 2025
Table 1 from Alternative Treatment of Osteoma Using an Endoscopic Holmium-YAG Laser18 fevereiro 2025 -
 1/72 Revell f22a. Decals are applied. It took some time but I'm happy. : r/modelmakers18 fevereiro 2025
1/72 Revell f22a. Decals are applied. It took some time but I'm happy. : r/modelmakers18 fevereiro 2025 -
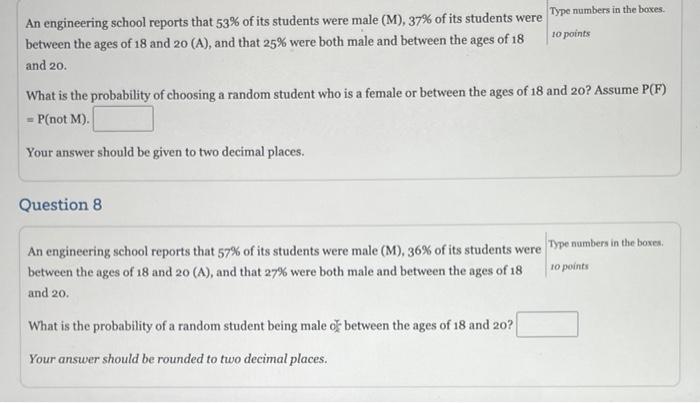
Solved An engineering school reports that 53% of its18 fevereiro 2025
-
 Image 127 of Connecticut - White Pages and Yellow Pages - New Haven - February 1878 thru October 189918 fevereiro 2025
Image 127 of Connecticut - White Pages and Yellow Pages - New Haven - February 1878 thru October 189918 fevereiro 2025 -
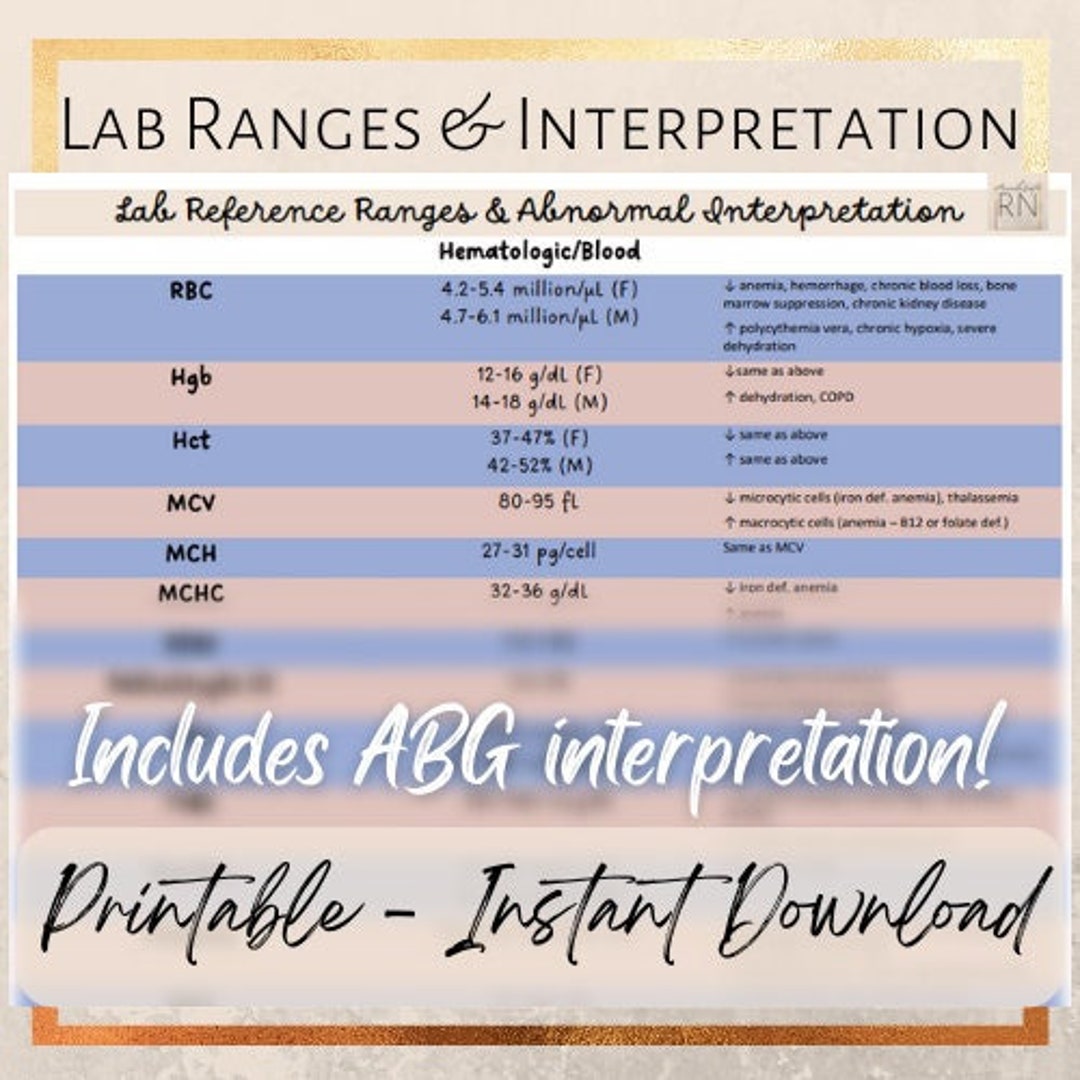 Lab Ranges & Interpretation Cheat Sheet18 fevereiro 2025
Lab Ranges & Interpretation Cheat Sheet18 fevereiro 2025
você pode gostar
-
 Emotion Letter B Alphabet Lore, Angry Latter Alphabet Lore | Poster18 fevereiro 2025
Emotion Letter B Alphabet Lore, Angry Latter Alphabet Lore | Poster18 fevereiro 2025 -
 Pokemon Videos on18 fevereiro 2025
Pokemon Videos on18 fevereiro 2025 -
![Gear up for the PlayStation Showcase 2023 [LIVESTREAM]](https://media.citizen.co.za/wp-content/uploads/2023/05/sony-playstation-2023.jpg) Gear up for the PlayStation Showcase 2023 [LIVESTREAM]18 fevereiro 2025
Gear up for the PlayStation Showcase 2023 [LIVESTREAM]18 fevereiro 2025 -
 Download Cut the Rope: Time Travel (MOD - Hints/Super Powers) 1.818 fevereiro 2025
Download Cut the Rope: Time Travel (MOD - Hints/Super Powers) 1.818 fevereiro 2025 -
 Al via le semifinali di Coppa Italia di Serie B 2023/2418 fevereiro 2025
Al via le semifinali di Coppa Italia di Serie B 2023/2418 fevereiro 2025 -
 fleetway sonic by kawaoa on Newgrounds18 fevereiro 2025
fleetway sonic by kawaoa on Newgrounds18 fevereiro 2025 -
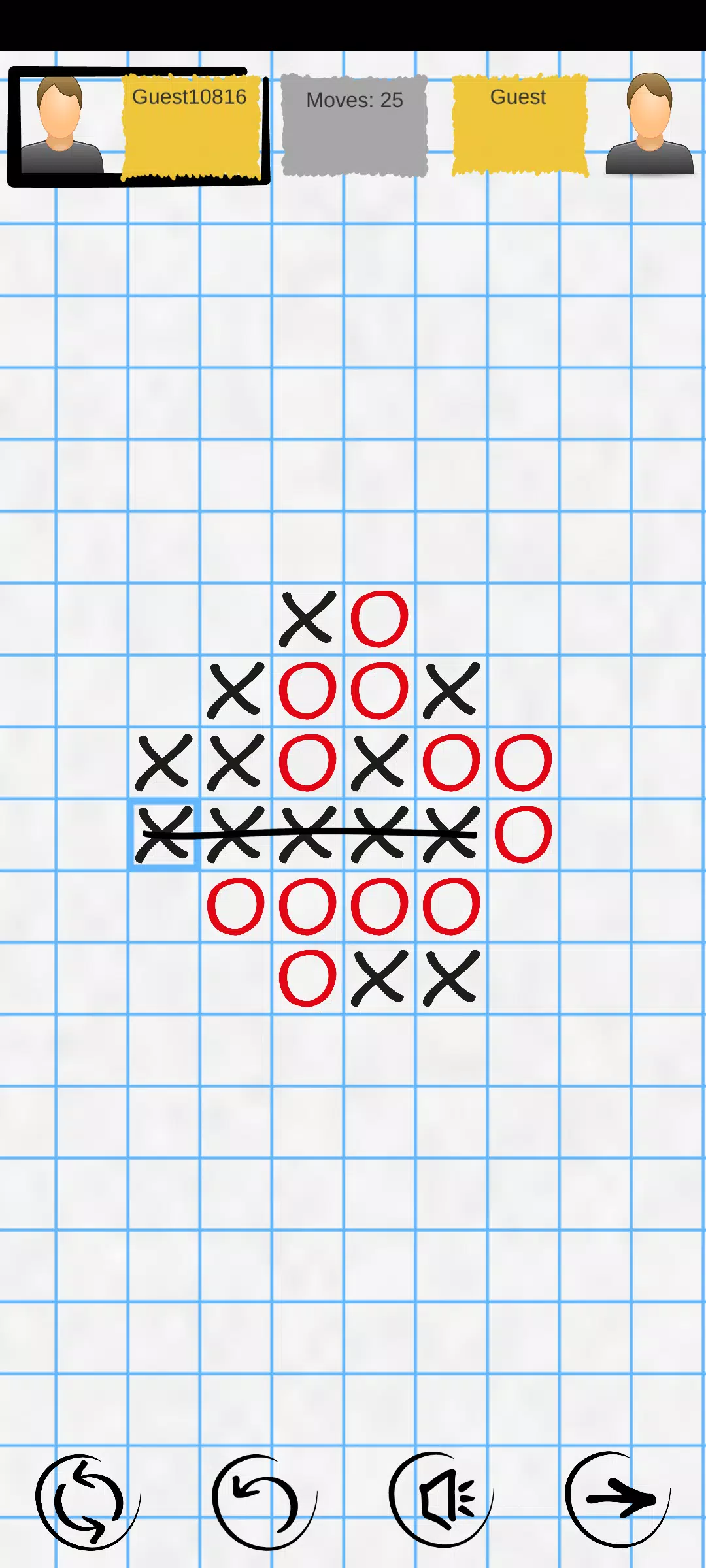 Tic Tac Toe Online: Mega XO APK for Android Download18 fevereiro 2025
Tic Tac Toe Online: Mega XO APK for Android Download18 fevereiro 2025 -
 Tapu Koko V, Pokémon18 fevereiro 2025
Tapu Koko V, Pokémon18 fevereiro 2025 -
 Gears of War 2 - GOTY Classic cover, Cover of Gears of War …18 fevereiro 2025
Gears of War 2 - GOTY Classic cover, Cover of Gears of War …18 fevereiro 2025 -
/cloudfront-us-east-1.images.arcpublishing.com/gray/KIZWGFWMIVJIVFYZCCOSPHKRW4.jpg) How to Watch Auto Racing Streaming Live Today - November 518 fevereiro 2025
How to Watch Auto Racing Streaming Live Today - November 518 fevereiro 2025